
 ALLISE
ALLISE  ARTERY
ARTERY
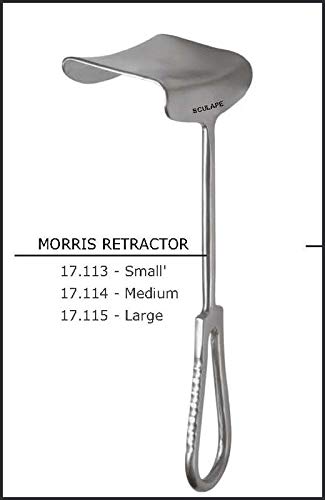 morrise retractor
morrise retractor 
 moynihans forcep
moynihans forcep  rightangle forcep
rightangle forcep 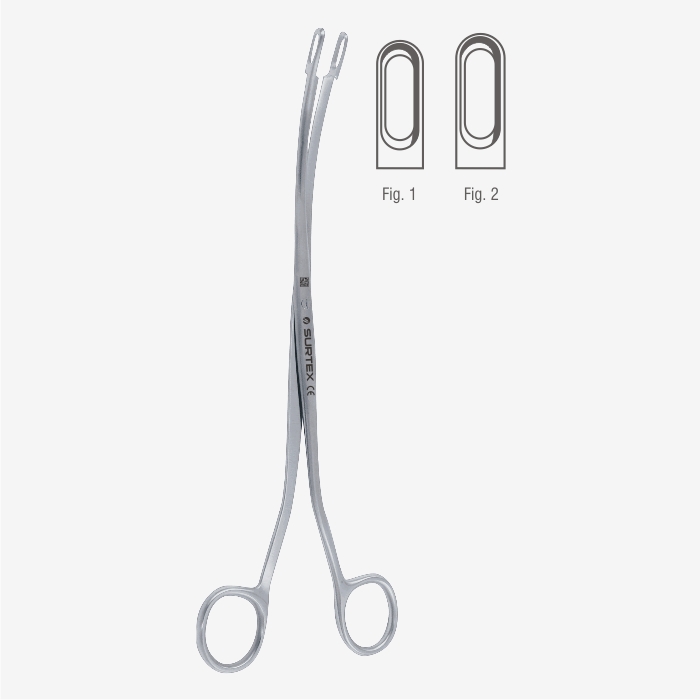 desgerdin forcep
desgerdin forcep


Standard of Practice II It is the responsibility of the HCWs to safely transport a patient to the preoperative holding area or operating room. Confirm IV lines, indwelling catheters, monitoring system lines and drains, and any other lines are secure and patent, and IV bag and collection containers are hanging away from the patient’s head.. Ensure head, arms and legs are protected, adequately padded, and patient is comfortable as possible. . The patient should be transported feet first; rapid movements, particularly when going around a corner should be avoided. Rapid movements, especially if the patient has received preoperative medications, can cause the patient to become disoriented, dizzy, and nauseated, and induce vomiting .. The staff person moving the transportation device should be positioned at the patient’s head in order to look forward for potential hazards. This also allows immediate access to the patient’s airway in case of respiratory distress or vomiting...
Hii i am Gourab Das , Medical Technologist , Diploma in Operation Theater Technology , Intern College of Medicine & Sagore Dutta Hospital . Formar MTOT MSDMCH MTOT Professional Running this Blog to help others as we are not find any proper guide for our studies time . Hope all of you guys enjoying this blog . Study , Stay safe , Be harder I also run another blog and youtube channel please share and subscribe to help others.
Comments
Post a Comment